Merry Christmas, Happy New Year
Australian Emergency Law wishes all my readers a very Merry Christmas and Happy New Year. I hope everyone who is on duty during this period can spend time with their family, as well as their emergency service family. I particularly acknowledge and thank the volunteers for the sacrifices they make, and will continue to make, over this period.
I’ll be spending some of my time catching up on some posts so if you have sent questions that haven’t been answered, keep watching this space.
Stay safe and enjoy whatever break you get.
Best wishes,
Michael Eburn.
{kind=link}
This blog is made possible with generous financial support from the Australasian College of Paramedicine, the Australian Paramedics Association (NSW), Natural Hazards Research Australia, NSW Rural Fire Service Association and the NSW SES Volunteers Association. I am responsible for the content in this post including any errors or omissions. Any opinions expressed are mine, and do not necessarily reflect the opinion or understanding of the donors.
Continued detention after apprehension by police – Mental Health Act 1987 (NSW) s 22
Today’s correspondent wants to revisit the Mental Health Act 1987 (NSW) s 22. They say:
… let’s imagine a situation where you work in a mental health unit in NSW. You observe that individuals are occasionally apprehended by the police under Section 22 and brought to the emergency department. After bringing the individual to the emergency department, the police leave the premises, leaving the care responsibility to the Emergency Department staff (i.e., doctors, nurses, and security guards).
The physicians in the emergency department, upon evaluating the individual, make a determination that the individual is mentally ill or mentally disordered and decide to transfer them to the mental health unit involuntarily. They believe that Section 22 alone allows for this transfer and the subsequent involuntary detention in the Mental Health Unit. They believe completing a Section 19 is unnecessary because they already have Section 22, even though the police officers have already left the premises. Additionally, they think that Section 22 remains valid for 24 hours, even if the police have already left the premises – so they believe they have 24 hours to complete a Section 19 and Form 1. They utilise Section 22 as the determination that the individual is mentally ill or mentally disordered, and to involuntarily detain that individual in the Mental Health Unit.
Only upon arrival at the mental health unit where you work, does the psychiatrist complete a Section 19 and Form 1. It’s important to note that sometimes, when the psychiatrist is on call, the individual may be involuntarily detained under Section 22 in the mental health unit for a duration of 30-60 minutes even without the presence of the police.
In this scenario, I am interested in understanding the correct course of action when an individual apprehended under “Section 22” is brought to the emergency department. Specifically, I would like to know if it is the duty of the emergency physicians to complete a “Section 19” and “Form 1” if they determine that the individual is mentally ill or mentally disordered, and require an involuntary admission to the mental health unit; specifically, completing a Section 19 and Form 1 before transferring them and admitting them to the Mental Health Unit. Furthermore, I am seeking clarification on the validity duration of “Section 22” after the departure of the police from the premises, as this information appears elusive within the Mental Health Act.
Section 22 provides that a police officer who ‘finds a person who appears to be mentally ill or mentally disturbed may apprehend the person and take the person to a declared mental health facility …’ provided certain conditions are met. Where the officer acts under s 22 the person is ‘apprehended’ so they are not free to go but must accompany the police to the mental health facility.
The emergency department is a declared mental health facilityI will first assume that the ‘emergency department’ is a declared ‘Mental Health Emergency Assessment’ facility (see NSW Health, Declared mental health facilities (21 August 2019)) and that the ‘physicians in the emergency department’ are authorised medical officers.
Once the person arrives at the facility, the staff at that facility may elect to detain the person (s 18). An authorised medical officer must examine the patient within 12 hours (s 27). The person can only be further detained if the authorised medical officer forms the opinion that ‘the person is a mentally ill person or a mentally disordered person.’ If that is the authorised medical officer’s opinion, the patient must be examined by a second doctor who must be a psychiatrist if the first doctor was not a psychiatrist. If that second doctor does not agree that the person is mentally ill or disordered, then there must be a third examination. If that third doctor agrees that the person is not mentally ill or disordered, then they must be released. If they are of the view that the person is mentally ill or disordered, they may be further detained and put before the Mental Health Review Tribunal (s 27).
There is no need for a doctor to sign a certificate under s 19. Section 19 says:
A person may be taken to and detained in a declared mental health facility on the basis of a certificate about the person’s condition issued by a medical practitioner…
The person is already at a declared mental health facility and is being detained under s 18(1)(c). Completing a s 19 certificate would add nothing. Section 18 says a mental health facility may detain a person because they were apprehended by police or because a doctor has written a certificate under s 19. Either way the mental health facility has to the power to detain the person and take action under s 27.
Once the person is detained (s 18) and has been examined by an authorised medical officer. (s 27) that second examination must be arranged. Section 80 provides:
… a person detained in a mental health facility may be transferred from the mental health facility to another mental health facility or another health facility.
It follows that the ‘physicians in the emergency department’ (assuming it is a declared mental health facility) can transfer the patient to another mental health facility (presumably the mental health unit) for the second and if necessary third examination. There is no need for a s 19 form. Once the person has been examined by an authorised medical officer who forms the view that the person is mentally ill or mentally disordered, their detention under s 18 is now over and their continued detention is justified by s 27.
Upon arrival at the mental health unit the psychiatrist should examine the patient and if they are of the view that the patient is mentally ill or mentally disordered they must complete the Form 1 described in the Mental Health Regulation 2019 (NSW) Sch 1. The person’s detention may be continued (s 27(1)(e)) and they may be treated (s 29).
The emergency department is not a declared mental health facilityIf the emergency department is not a declared mental health facility, then the police officer’s decision does not justify detention at that centre. If the doctors there form the view that the patient is mentally ill or mentally disordered, they may transfer the person to a mental health facility (s 25).
Any such person is taken to have been detained in the declared mental health facility under section 19 when the person is transferred to the facility.
In those circumstances the doctor does not need to complete a s 19 certificate as teh person is ‘taken to have been’ detained as if a s 19 certificate had been completed. That works if the person agrees to the transfer. If the person does not agree to the transfer, then a doctor would have to complete a s 19 certificate to authorise a NSW Health employee, ambulance officer or police officer to take the person to the mental health facility (ss 19 and 81).
SummaryIf the emergency department is a declared mental health facility
- Police form the necessary views under s 22.
- Staff at the mental health emergency assessment facility may detain the person (s 18(1)(c)).
- Within 12 hours the person must be examined by an authorised medical officer (s 27(1)(a)).
- If the medical officer forms the opinion that the person is mentally ill or mentally disordered, their detention may be continued pending a second, and if necessary, third examination (s 27(1)(b) and (c)).
- If the opinion is confirmed by the 2nd, or if necessary, the 3rd doctor, the person may be detained pending review by the Mental Health Review Tribunal (s 27(1)(d) and (e)).
If the emergency department is not declared mental health facility
- Police bring the person to the hospital.
- The doctor forms the view that the person is mentally ill or mentally disordered.
- They can transfer the person to a mental health facility and the person is deemed to have been detained under s 19.
- If the person refuses, the doctor would need to complete a s 19 certificate to authorise NSW Health staff, ambulance officers and, in some cases, police to transport the person to a declared mental health facility.
To return to the question posed:
- If police act under s 22 they can leave the individual in the care of the emergency department staff (see Who is detaining the person – the police or the mental health facility (NSW) (December 3, 2023).
- If the ‘physicians in the emergency department’ are authorised medical officers and determine that the individual is mentally ill or mentally disordered, they can transfer the person to another mental health facility (s 80). Completing a s 19 is unnecessary because, at that point the detention and transfer is justified by ss 27 and 80. Section 22 is no longer relevant, but neither is s 19.
- Where a person is being detained under s 18(1)(c), ie on the basis that the person has been brought to a mental health facility by police acting under s 22, that detention can be for 12 hours, but there is no requirement for to police to remain. The detention for up to 12 hours is valid ‘even if the police have already left the premises’. The detention under s 18(1)(c) ends when the person is examined by an authorised medical officer who either forms the view that the person is not mentally ill or mentally disordered in which case they must be released (s 27(1)(a)), or does form the view that the person is mentally ill or mentally disordered in which case their ongoing detention is authorised by s 27(1)(b).
- Upon arrival at the mental health unit the psychiatrist does not complete a s 19 certificate. If the psychiatrist does form the view the person is mentally ill or mentally disordered, he or she must complete the form provided for in the regulation. That is not the same as the s 19 certificate. The psychiatrist has to see the person ‘as soon as possible’ (s 27(1)(b)). Once the person is brought to the mental health facility they are detained by that facility, not the police so there is no need for the police to still be there.
- It is not the duty of the emergency physicians to complete a “Section 19” and “Form 1” if they are authorised medical officers. They would need to do that if the emergency department is not a declared mental health facility, and they are not authorised medical officers.
- Section 22 is not relevant after police have delivered the patient. Section 22 authorise the police to apprehend a person. They take them to the mental health facility and the facility then detain the person under s 18(1)(c). That detention is justified because the person was brought to the facility ‘after being apprehended by a police officer’. The police apprehension is now over, so the detention remains valid even after the police have left.
This blog is made possible with generous financial support from the Australasian College of Paramedicine, the Australian Paramedics Association (NSW), Natural Hazards Research Australia, NSW Rural Fire Service Association and the NSW SES Volunteers Association. I am responsible for the content in this post including any errors or omissions. Any opinions expressed are mine, and do not necessarily reflect the opinion or understanding of the donors.
Legal error in reporting on NSW paramedic registration bans No. 2
Following my post, Legal error in reporting on NSW paramedic registration bans (December 5, 2023) I received the following as a question/comment via Facebook, but I’ve decided to give a detailed answer as a post in its own right.
It is my understanding that when registration for paramedics in Australia was implemented, it required the passage of National Law legislation in each state to bring registration into effect (please correct me if I’m wrong). Out of interest, is there any legal reason that would prevent the NSW government from modifying this legislation such that registration would no longer be required for NSW paramedics? Obviously would possibly not reflect well on the government from a public relations perspective, but just wondering what options are open to them if paramedics opt not to register come the end of December.
It’s true that the national law is not really a national law at all, it is the same (or more accurately a similar) law passed in each jurisdiction to create a national scheme. It follows that NSW could pass amendments to the law as it applies in NSW. But I’m not sure why it would bother, even though the NSW government is threatening to do just that – see Michael McGowan and Laura Banks, Paramedic pay dispute threatens NYE emergency response, Sydney Morning Herald, 8 December 2023, which says:
… with thousands of paramedics threatening not to renew their registrations by the end of the year, he [NSW Health Minister Ryan Park] did not rule out taking the dramatic step of recalling parliament from its summer break to pass legislation to break the deadlock….
Park would not go into detail on what that legislation might look like, but said it could change rules to allow paramedics to work without registration.
People cannot call themselves, or be called, paramedics without registration but there is no law that says people who are not paramedics cannot work in ambulance services or provide advanced patient care. Registration is required for people who call themselves paramedics, but it’s not required for ‘ambulance drivers’.
An issue is not only must a person not hold themselves out as a paramedic (s 113(1)), but their employer must also not hold them out as a paramedic (s 113(2)) and that could see ASNSW in breach if it holds out that its dispatching paramedics if they’re not registered (eg by having ‘paramedic’ written on their cars). As I said in my earlier post that is probably avoidable by having an HSU member paired with a person who has renewed their registration.
As for drugs, the Poisons and Therapeutic Goods Regulation 2008 (NSW) Appendix C cl 7 says:
A person–
(a) who is employed in the Ambulance Service of NSW as an ambulance officer or as an air ambulance flight nurse, and
(b) who is approved for the time being by the Secretary for the purposes of this clause,
is authorised to possess and use any Schedule 2, 3 or 4 substance that is approved by the Secretary for use by such persons in the carrying out of emergency medical treatment.
Similar wording is used in r 101 relating to s8 drugs.
Those provisions don’t refer to paramedics, they refer to ambulance officers. What is relevant is the terms of any authority issued under paragraph (b). If the approval is made to people personally, ie by name, there is no issue. If it is made by reference to position – eg ‘ambulance paramedic’, ‘critical care paramedic’, ‘intensive care paramedic’ etc then presumably an unregistered person is no longer a paramedic so no longer fits the description of an authorised ambulance officer. But that could be resolved by changing the terms of the authorities rather than any legislative change.
The final issue, as I see it, is an industrial one and whether it is an essential part of one’s job to be a paramedic (see Potential consequences of proposed NSW Ambulance industrial action (September 16, 2023)). In that post I referred to the Paramedics and Control Centre Officers (State) Award 2022 (28 July 2022) and noted that:
It doesn’t specifically say that the person has to be registered with the Paramedicine Board but I think that can be implied given that only a registered person can use the title ‘paramedic’.
If registration is an essential part of the job then, I argued, fail to renew registration may amount to abandonment of employment, but that is not automatic. That may give ASNSW the option to terminate a person’s employment, but it doesn’t mean they have to, they could continue to employ their current staff, but not call them paramedics. It really does depend on an interpretation of the award, the detailed job descriptions, and employment contracts and what they say about maintaining registration. I do not have access to those details so can say no more than it is possible that ASNSW could seek to terminate a former paramedic’s employment if they fail to renew their registration by 31 December.
ConclusionThe NSW government doesn’t have to change the law to allow ‘paramedics to work without registration’. Rather it would have to change the law to allow people to be called paramedics who are not registered or, and this would be legally easier, admit to the people of NSW that it is staffing its ambulance with a mix of workers, some of whom are paramedics and some of whom are not. It need not affect the level of service but would affect the regulatory environment for those non-paramedics who continue to work as ambulance drivers.
This blog is made possible with generous financial support from the Australasian College of Paramedicine, the Australian Paramedics Association (NSW), Natural Hazards Research Australia, NSW Rural Fire Service Association and the NSW SES Volunteers Association. I am responsible for the content in this post including any errors or omissions. Any opinions expressed are mine, and do not necessarily reflect the opinion or understanding of the donors.
New legislation for Queensland SES
I’m asked if I have ‘any thoughts on the proposed legislation for the Qld SES? In particular how does it compare to the other states and territories?’ The Bill is the State Emergency Service Bill 2023, introduced to the Parliament on 28 November 2023.
I’m not going to go through the bill section by section. With a brief overview it looks consistent with legislation in other states and territories. Nothing ‘jumps out’ as a great innovation or a bizarre departure from standard, with one exception.
The Act provides for a Commissioner, who will be responsible for (s 9):
(a) the establishment of SES units and the designation of areas for SES units; and
(b) the appointment of persons as SES chief officer, local controllers, SES commanders and other SES members; and
(c) the establishment of management and support services for the SES; and
(d) the development of policies to help the SES perform its functions effectively and efficiently including, for example, policies about training SES members; and
(e) the giving of directions and guidance to the SES chief officer, local controllers, SES commanders and SES members; and
(f) the performance of any other function relating to the SES that is given to the commissioner under this Act or another Act.
The Chief Officer, appointed by the Commissioner is (s 13):
(a) to manage the SES in a way that ensures the SES operates effectively and efficiently;
(b) to comply with any direction given by the commissioner that is relevant to—
(i) the functions of the SES chief officer or the SES; or
(ii) SES members;
(c) to perform any other function relating to the SES given to the SES chief officer under this Act or another Act.
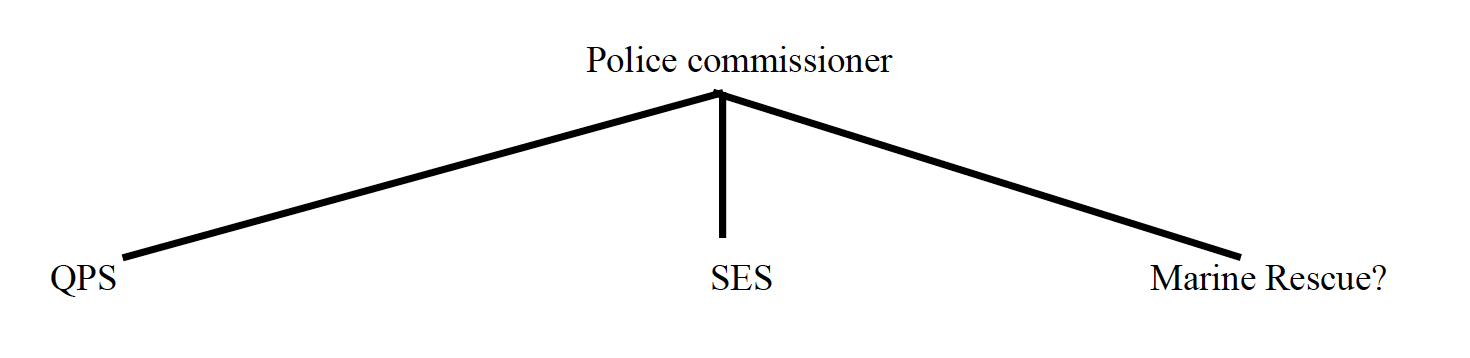
In another post – Status of Queensland Rural Fire Brigades (September 10, 2014) I said:
We can describe the relationship as three services, all lead by the same Commissioner, but not the same service.
{kind=link}
Under the new system the diagram will be similar but it will be the police commissioner at the top:
{kind=link}
Having a single commissioner is not unique, for example the emergency services in the ACT are led by the Emergency Services Commissioner with each service having a chief officer. In Victoria there is the Emergency Management Commissioner. In Western Australia the Fire and Emergency Services Commissioner exercises functions for the SES, Volunteer Marine Rescue as well as the urban and rural fire brigades.
What is unique for Queensland is that it is the police commissioner taking on thise role. Personally, I think of police as law enforcement. If we accept that emergency management is itself a professional role – extending beyond response – then it seems more fitting to have an emergency management commissioner rather than a police commissioner at the top of the pyramid.
In a submission to the inquiry into the 2022 NSW floods, the NSW Police Association said (emphasis added):
We submit there should be one agency always responsible for the control and coordination of emergency response operations. The consistent performance of this role by the same agency will ensure there is no ambiguity regarding who is in control; it is not dependent on circumstances and therefore no confusion over who is controlling and coordinating operations. It also means that agency will have the greatest level of experience and knowledge to perform the role in all emergency situations.
The NSWPF is best placed to perform that role.
The Fire Brigade Employees Union (the FBEU) took a different view. They submitted that (emphasis added):
The FBEU maintains that the most appropriate agency to undertake this work is FRNSW as they have the capability and structures in place to deliver the required response functions in emergencies of this nature.
It appears that Queensland has experimented with having the SES as part of a larger Fire and Emergency Service but is now shifting to have it as part of an expanded police and emergency service. Whether either is a better fit, or whether the SES should (as it currently does in NSW) stand alone remains to be seen.
This blog is made possible with generous financial support from the Australasian College of Paramedicine, the Australian Paramedics Association (NSW), Natural Hazards Research Australia, NSW Rural Fire Service Association and the NSW SES Volunteers Association. I am responsible for the content in this post including any errors or omissions. Any opinions expressed are mine, and do not necessarily reflect the opinion or understanding of the donors.
RFS taking action on land controlled by a transport authority
Today’s correspondent says:
On 28/2/23 you published a post titled “Power of NSW RFS to close roads owned or managed by Transport for NSW”.
As a Deputy Captain in the NSW RFS, I thought the identified gap in RFS powers should be addressed, so I communicated it through the RFSA, making reference to your post.
Pleasingly, the Government has responded in the Emergency Services Legislation Amendment Bill 2023, which has passed both houses and is ready for assent.
The new Bill returns the power for an RFS officer to close TfNSW-managed streets or public places without permission, subject to a requirement to notify TfNSW as soon as practicable after the closure.
Revisiting the issue and reading the follow-up posts on your website today, has made me aware that it is not just the power to close streets and public places that is removed for TfNSW land. It is all RFS functions and powers under Division 3 of the Rural Fires Act. I doubt it was ever the Government’s intention to require the RFS to obtain TfNSW permission before dealing with fires and other incidents on TfNSW streets and land.
I think the effect of the legislative change needs to be broadened by replacing the words ‘functions conferred by section 24” with “functions conferred by this Division” in both 27(2) and 27(3).
I have communicated this broader concern within the RFSA, and would be interested in your opinion on the matter.
I’m pleased to think I may have made some contribution to changing the law.
- Details of the Bill can be found here: https://www.parliament.nsw.gov.au/bills/Pages/bill-details.aspx?pk=18506
- The Explanatory memoranda is here: https://www.parliament.nsw.gov.au/bill/files/18506/XN%20Emergency%20Services%20Legislation%20Amendment%20Bill%202023.pdf
- And the Minister’s 2nd reading speech is here: https://www.parliament.nsw.gov.au/Hansard/Pages/HansardResult.aspx#/docid/’HANSARD-1323879322-135946‘
The relevant provision is the new s 27. The Bill will take effect on the day it receives royal assent (s 3). When that happens s 27 of the Rural Fires Act 1997 (NSW) will say:
27 Permission needed from transport authorities for exercise of certain functions
(1) Subject to subsection (2), the functions conferred by this Division may not be exercised in relation to land or property vested in, or under the control of, a transport authority without the permission of—
(a) the transport authority, or
(b) a person authorised by the transport authority.
(2) The functions conferred by section 24 may be exercised in relation to land or property vested in, or under the control of, Transport for NSW without the permission of Transport for NSW, unless—
(a) the land or property is land or property on which rail services are provided, or
(b) rail services would be affected by the exercise of the functions in relation to the land or property.
(3) If a function conferred by section 24 is exercised in relation to land or property vested in, or under the control of, Transport for NSW without the permission of Transport for NSW that results in a street being closed to traffic, a member of the Service must, as soon practicable after the closure, advise Transport for NSW about the closure.
(4) In this section— transport authority means the following—
(a) NSW Trains,
(b) Rail Corporation New South Wales,
(c) Rail Infrastructure Corporation,
(d) Residual Transport Corporation of New South Wales,
(e) Sydney Metro,
(f) Sydney Trains,
(g) Transport for NSW,
(h) Transport Infrastructure Development Corporation.
Section 24 is the power to ‘cause any street or public place in the vicinity of a fire, incident or other emergency to be closed to traffic.’ The officer in charge of the RFS will be able to close any street or public place provided that it is not on land where rail services are provided or will affect the operation of a rail service.
But as my correspondent notes there are other powers under Part 2, Division 3. One is the power to enter premises. Section 23 says:
An officer of a rural fire brigade or group of rural fire brigades may enter any premises for the purpose of exercising any function conferred or imposed on the officer by or under this Act.
But not, it seems, premises ‘vested in, or under the control of, a transport authority’. So the RFS cannot force entry to a train station in order to extinguish a fire, or an office block with the headquarters of TfNSW. Again one can imagine that the rail authorities may not want RFS forcing entry to a rail corridor or even, perhaps, a signal box because of the dangers in the system that require expert knowledge. In the city TfNSW may even maintain a specialist emergency service – see Operating a “Rail Emergency Response Unit” (November 20, 2016) but that’s hardly helpful given the extent of operations of the Rural Fire Service.
Other things the RFS can do under Division 3 are make premises safe (s 25), use water and works (s 26), remove persons or obstacles (s 22A) or ‘take any other action that is reasonably necessary or incidental to the effective exercise’ of an RFS function (such as fighting fires), but due to the new s 27, the RFS will not be able to exercise any of these powers on ‘land or property vested in, or under the control of, a transport authority’ without the permission of that authority.
That is truly bizarre.
Rather than refer to ‘functions conferred by this Division” in both 27(2) and 27(3)’ I would, if the section were essential, rewrite it to say:
27 Permission needed from transport authorities for exercise of certain functions
(1) The functions conferred by this Division may not be exercised in relation to land or property vested in, or under the control of, a transport authority without the permission of—
(a) the transport authority, or
(b) a person authorised by the transport authority.
if
(c) the land or property is land or property on which rail services are provided, or
(d) rail services would be affected by the exercise of the functions in relation to the land or property.
(2) In this section— transport authority means the following—
(a) NSW Trains,
(b) Rail Corporation New South Wales,
(c) Rail Infrastructure Corporation,
(d) Residual Transport Corporation of New South Wales,
(e) Sydney Metro,
(f) Sydney Trains,
(g) Transport for NSW,
(h) Transport Infrastructure Development Corporation.
But even that would be bizarre as it would still limit the power of the RFS to say evacuate a train station in order to try and fight a fire burning in the train station. Rather than try and rewrite the section someone – in particular TfNSW and the RFS – should work out exactly what is required and if it is that the RFS should not enter a rail line without first telling TfNSW to make sure the trains are stopped, then that is what it should say.
This blog is made possible with generous financial support from the Australasian College of Paramedicine, the Australian Paramedics Association (NSW), Natural Hazards Research Australia, NSW Rural Fire Service Association and the NSW SES Volunteers Association. I am responsible for the content in this post including any errors or omissions. Any opinions expressed are mine, and do not necessarily reflect the opinion or understanding of the donors.
Protest first aid volunteers
Today’s correspondent:
… recently started volunteering with Melbourne Street medics who attend rallies in the city to provide first aid. The group is a bunch of volunteers who have first aid training, wear green vests [see photo below, supplied], and have been trained on decontamination of pepper spray. There is no formal organization or contract to provide care, it is all organized in a group chat and we all just turn up.
{kind=link}
A recent discussion came up regarding providing care to counter protesters, and what obligation you would have (if any). Traditionally you wouldn’t have a Duty of Care as you are just a bystander. I believe that as you are putting on a green vest and identifying as a medic, that would change, and you would have a Duty of Care, despite the lack of formal contact
One can infer that the group is not ‘medics who attend rallies in the city to provide first aid’ for everyone, rather they are ‘medics who attend rallies … to provide first aid to supporters of a particular cause’. If that were not the case the issue of ‘counter protestors’ would not arise nor would the issue of who to treat. If they were there with the express intent of providing first aid at the rally it would be for everyone there.
But that’s fine. If someone is organising a rally then people who support that cause are allowed to go and express their support. And if some of them want to identify as being trained in first aid and are part of that rally they can provide first aid to those on the side they support, in the same way that marshals will be there to marshal their side of the rally, not any counter protestors. And it is highly appropriate for anyone organising such an event to think about the provision of first aid and security services as part of the event organisation.
So does that give rise to a duty of care to others, particularly in the context of ‘no formal organization or contract to provide care, it is all organized in a group chat and we all just turn up’? I don’t think so.
Mere foreseeability that someone may get injured or that someone who is injured would benefit from first aid is not sufficient to give rise to a duty of care. Stuart v Kirkland-Veenstra [2009] HCA 15 confirmed that there is no duty to come to the rescue of others. In that case there was discussion that organisations, such as police, may have special statutory powers and duties that could give rise to a duty to exercise those powers or perform those duties but that cannot be relevant here.
The ‘counter-protestors’ could not argue that they had any reasonable reliance on the ‘Melbourne Street medics’ unless there was a meeting between potential protest groups and police to plan the day and one side said ‘well have first aiders there, to look after everyone’. And the first aiders are presumably turning out because a cause they support is organising the event. It might be different if they really were a-political and decided to set up a first aid post in Federation Square simply because they knew there would be a crowd there or because they were there every weekend and the protest just happened to be there – but to repeat what I said before – if that were the case the concept of a ‘counter-protest’ would not be relevant as they would not be there to support one side, over the other.
An employer has to have arrangements in place for first aid at the workplace (WorkSafe Victoria Compliance code: First aid in the workplace (2021)). It would not be reasonable for one employer to say ‘My business is co-located with other businesses and one of them has a first aider so I’m just going to rely on that person’. That would not impose a duty on the second business to provide first aid services to the first nor relieve the first employer of their obligations. By analogy, the fact that one side of a rally has first aiders would not impose a duty on those people to render care to the ‘other’ side.
Justice is a fundamental principle of bioethics and health care codes of practice. We would expect Ambulance Victoria as well as the staff of the public hospitals to treat anyone who comes to them based solely on their clinical need and without regard to the side of the protest they were supporting. There is the ethical issue of whether a first aider should walk past a person who they may be able to assist but that would not, in this context, give rise to a legal duty. In extreme cases, such as cardiac arrest, one would hope that anyone would stop and assist if they could, regardless of the person’s stance on any issue, but that would not give rise to a legal duty on a person with a first aid certificate just because they had a first aid certificate.
Even if there is a duty, the duty is to only do what is reasonable. Before a person could or should assist, regard must be had to the nature of the event. It may not be safe for someone who clearly identifies with one cause to become ‘embedded’ in the ‘other side’. If you’re protesting for trans-rights, you may rightly be uncomfortable and unsafe stopping to assist a balaclava wearing, Nazi-saluting counter protestor. Equally if the first aiders are there as part of the anti-drag story time protest at the local library, they may not feel comfortable or safe trying to provide care to the local drag queen and her supporters.
Finally in any legal action in negligence a plaintiff has to prove the breach of duty caused damage. If a person has been sprayed with OC it is the OC that is causing their damage, not the action of the first aider. Failing to stop does not make the situation worse, it fails to make it better and there is, to return to where we started, generally no duty to do that. Also the protest first aid group are not the only people who can assist. The protestors will be assisted by police and can be assisted by Ambulance Victoria and people in their own group. There is no reasonable grounds to rely on the volunteers and they are not the best placed to provide the care required.
ConclusionThere is no duty to rescue. A group of people who identify that they have first aid training and who turn out clearly in support of, and as part of a particular group would not be under a legal duty to come to the aid of others who are clearly opposed to their event in the dynamic circumstances of an ongoing protest and were stopping to assist may not be safe.
It could be different if they were clearly members of an a-political organisation that really was there to provide care to everyone.
There may be ethical issues and one has to live with oneself particularly if you are planning to walk past a person who asks for help or who you think may die without help, but ethical issues do not always translate to legal duties.
This blog is made possible with generous financial support from the Australasian College of Paramedicine, the Australian Paramedics Association (NSW), Natural Hazards Research Australia, NSW Rural Fire Service Association and the NSW SES Volunteers Association. I am responsible for the content in this post including any errors or omissions. Any opinions expressed are mine, and do not necessarily reflect the opinion or understanding of the donors.
Can paramedics work in hospitals?
Today’s correspondent asks
Why can’t paramedics work in hospitals? In clinical roles
Apparently there are legislative reasons.
There are no legislative reasons. Hospitals could employ paramedics in clinical roles if hospitals wanted to create clinical roles for paramedics. They would not doubt have to negotiate with the nurses and doctors to do so, but they could do it if they saw a benefit.
This blog is made possible with generous financial support from the Australasian College of Paramedicine, the Australian Paramedics Association (NSW), Natural Hazards Research Australia, NSW Rural Fire Service Association and the NSW SES Volunteers Association. I am responsible for the content in this post including any errors or omissions. Any opinions expressed are mine, and do not necessarily reflect the opinion or understanding of the donors.
Legal error in reporting on NSW paramedic registration bans
An article from the Sydney Morning Herald (Laura Banks, ‘Paramedics will shut down triple 0’: Boycott to go ahead as pay negotiations stall’(December 1, 2023)) about the HSU’s registration ban industrial action (see Potential consequences of proposed NSW Ambulance industrial action (September 16, 2023)) says ‘Without registration, paramedics are legally unable to attend triple zero calls.’
That is not the law. NSW Ambulance responds untrained volunteers (NSW Ambulance and GoodSAM App (November 26, 2023)) and non-paramedic clinical volunteers (https://www.ambulance.nsw.gov.au/get-involved/volunteer) to triple zero calls. There is no law that says who can and who cannot attend triple zero calls.
What the Health Practitioner Regulation National Law says, at s 113, is that a person who is not registered cannot use the title ‘paramedic’ and cannot be held out to be a paramedic. That may cause problems for NSW Ambulance if non-registered people respond in ambulances marked ‘paramedic’ or in circumstances where the people receiving care expect that the person on the door is a paramedic. That may indeed be solved by HSU members wearing their red ‘NSW Ambulance Driver’ t-shirts and being paired with a paramedic who is not taking part in the action.
There is no doubt that this action poses a considerable threat – both operationally and from a public relations perspective – to NSW Ambulance and the government and is no doubt bringing pressure on the government to come to the table to meet the paramedics’ demands. There may be legal reasons why employees who have not renewed their registration cannot do things that NSW Ambulance employment standards assume will be done by paramedics (in particular supply and administer scheduled drugs), but it is not the case that without registration they are ‘legally unable to attend triple zero calls.’
This blog is made possible with generous financial support from the Australasian College of Paramedicine, the Australian Paramedics Association (NSW), Natural Hazards Research Australia, NSW Rural Fire Service Association and the NSW SES Volunteers Association. I am responsible for the content in this post including any errors or omissions. Any opinions expressed are mine, and do not necessarily reflect the opinion or understanding of the donors.
‘No transport, no drugs’ – is that a rule?
Today’s correspondent is ‘… a fairly junior paramedic working for the Queensland ambulance service (QAS)’ who hopes I can provide:
… some clarity surrounding medication safety law/guidelines.
Specifically, my question relates to registered paramedics providing medications (S4s/S8s) to patients and the patient’s right to refuse transport / further clinical monitoring – or a paramedics responsibility with providing this form of treatment with the knowledge that this patient will likely refuse transport after treatment is provided.
This question comes from the general consensus among many clinicians and both university educators being that we (paramedics) should not provide medications or refuse to administer medications if the patient is likely going to decline transport to hospital. In general this refers more specifically to comfort care such as antiemetic or analgesia type medication management, opposed to life saving medication such as adrenaline.
My immediate thought was ‘what’s the issue?’ If my doctor prescribes schedule 4 drugs I go to a chemist, get the script filled and go home and take the drugs – no-one’s supervising me so the issue cannot arise just because the drugs are schedule 4. And whilst I’ve not been prescribed s 8 drugs, I can imagine that in many cases they are taken by people without supervision. I asked my correspondent to give further details and they replied:
I was thinking more along the lines of the liability associated with Ondansetron as an S4, and administering it on a non-transport job and if there are different legal considerations for IM vs Oral routes.
But am also curious of your opinion for S8s in the same manner say for IM Morphine or IHL methoxyflurane – where these have been administered as analgesia but then the patient decides they want to decline transport after since they’re pain is now controlled.
(The links above are to the relevant Queensland Ambulance Drug Therapy Protocols. I note methoxyflurane is S4, not S8; see Therapeutic Goods (Poisons Standard—October 2023) Instrument 2023 (Cth)).
I infer the question relates to ‘comfort care such as antiemetic or analgesia type medication management, opposed to life saving medications such as adrenaline’ because a person who needs adrenaline for the treatment of the conditions listed in the QAS Drug Therapy Protocols: Adrenaline (Epinephrine) (DTP_ADR_0323, March 2023); that is:
- Cardiac arrest
- Anaphylaxis or severe allergic reaction
- Severe life-threatening bronchospasm or silent chest
- Shock unresponsive to adequate fluid resuscitation
- Bradycardia with poor perfusion [or]
- Croup
is unlikely to be able to or refuse treatment, but is that necessarily so? A person with a severe allergic reaction may, I assume, respond rapidly to the treatment, and then decline further treatment and transport. If that’s correct, I’m not sure why the distinction between ‘comfort care’ and ‘life saving medication’ is relevant.
In any event let’s now turn to the issues raised.
First, if a patient is given a drug and then refuses further treatment or transport there is nothing the paramedics can do about that. A person can refuse treatment at any time. They are not compelled to comply with paramedic directions because they complied a moment ago. Consent is a process not a single step and can be withdrawn at any time.
Second, if the patient ‘will likely refuse transport after treatment is provided’ I fail to see how that would be grounds for withholding the treatment they consent to. One of the principles of bioethics is ‘justice’ which in simple terms is about giving people what they need on the basis of need rather than other, irrelevant considerations. In this case none of the Drug Therapy Protocols suggest for example that the drugs should only be given when patients can be monitored or that the administration of the drugs necessitates some hospital only follow up. If you give a person an anti-emetic or analgesia so they can then follow up with out of hospital care, or perhaps attend to a pressing need (like making arrangements for their children) and then make their own way to hospital, haven’t you provided a valuable service to the patient, the health system and the community?
Given that methoxyflurane lasts for 5-10 minutes there may be a fear that the person thinks the pain is relived but if you go they’ll call you back when the drug wears off. That is no reason not to give the drug and it is no warrant to force the person to accept transport. You tell the patient, and ‘go slow’ on the pack up until they realise that no, whatever was hurting before, still hurts.
Finally there is the circumstance where the patient has made it clear that they are not going to accept transport but are willing to accept care on the scene. That may be an issue with a drug like morphine in that it can cause bradycardia, respiratory depression, nausea and vomiting, hypotension and drowsiness. They may all be problems if the patient is left alone.
There could certainly be an argument that you could say to a patient ‘if you’re not going to come with me I cannot give you this drug, because of its dangerous potential side effects’. I cannot see how that arises with the other drugs listed (at least from what I can infer from the drug protocols) and it doesn’t change the fact that even if they agree, once you have given the drug, they can then refuse further transport and there is nothing you can do to force them if they remain competent to make the decision.
ConclusionThere is no legal reasons to conclude that paramedics ‘should not provide medications or refuse to administer medications if the patient is likely going to decline transport to hospital’. As paramedics you are there to deliver health care, the days of just being a transport service are over. You deliver care to the patient based on the patient’s needs often with the hope that the care you deliver will mean they don’t need further transport to hospital.
There may be an argument with respect to some drugs that you should not administer them if you think the patient needs to be monitored afterwards given the drugs possible side effect but even with morphine that could be met by telling their family or friends – ‘they don’t want to come with me, but look out for these symptoms and call us back if any of these things happen’.
The law asks you to act reasonably in all the circumstances which includes making clinical judgements such as whether the risks to the patient outweigh the benefits where the patient has made it clear that they are going to refuse further transport. There is however no law that says ‘no transport, no drugs’ and it would appear to me (recognising that I am not a clinician) that for most drugs that is not an issue. A blanket rule of ‘no transport, no drugs’ would be the antithesis of good health care.
This blog is made possible with generous financial support from the Australasian College of Paramedicine, the Australian Paramedics Association (NSW), Natural Hazards Research Australia, NSW Rural Fire Service Association and the NSW SES Volunteers Association. I am responsible for the content in this post including any errors or omissions. Any opinions expressed are mine, and do not necessarily reflect the opinion or understanding of the donors.
Suspended QAS paramedic wins right to continue to be paid pending the outcome of criminal charges
Mark Roche was an advanced care paramedic who remains employed by the Queensland Ambulance Service (QAS). On 30 December 2022, he was charged with a criminal offence. The Queensland Police Service (QPS) advised the ambulance service and on 3 January 2023 Mr Roche was suspended on full pay pending determination of the criminal allegations.
On 6 March 2023 the Health Ombudsman took immediate action under the Health Practitioner Regulation National Law to suspend Mr Roche’s registration. On 24 March the QAS terminated Mr Roche’s suspension on full pay. They did not however suspend him without pay, rather the relevant decision maker wrote:
I have formed the view that the suspension of your paramedicine registration prevents you from not only performing the inherent requirements of your role as a paramedic, it also restricts you from performing any other role within the Queensland Ambulance Service (QAS) that impacts on the delivery of services.
Mr Roche was invited to use up available leave balances pending the finalisation of the allegations against him.
Mr Roche appealed against the decision to terminate his suspension with pay to the Queensland Industrial Relations Commission – Roche v State of Queensland (Queensland Ambulance Service) [2023] QIRC 334 (28 November 2023). The case was complicated by the fact that during the time between his first suspension and subsequent decisions, various suspension provisions in the Ambulance Service Act 1991 (Qld) were repealed and replaced by provisions Public Sector Act 2022 (Qld). The question before the Commission was (at [18]) whether the decision was ‘fair and reasonable’. A decision to suspend an employee on full pay did not require consideration of ‘natural justice’ but a decision to suspend an employee without pay did ([37]). The final outcome of suspension ([37]) is to be:
- suspension is lifted and the employee returns to normal duties, or
- suspension is lifted and management or discipline action is taken, or
- suspension is lifted during or at the conclusion of a disciplinary process, or
- the employee separates by resignation or termination.
The appellant, Mr Roche, argued that the decision was in effect to suspend him without pay and this was not reasonable because (at [41]):
- He is entitled to the presumption of innocence;
- QAS failed to consider, as they were required to consider, whether he could ‘work in alternative area of QAS (eg Fleet) or undertake host employment in other government agencies or departments’;
- He was denied ‘procedural fairness’ in that he was not invited to show cause why the decision to terminate his suspension on pay should not have been made.
- Resultant financial hardship and emotional distress
Commissioner McLennan upheld Mr Roche’s appeal.
When he had been suspended under the Ambulance Service Act had had been advised that the grounds for suspension were that he was ‘liable to discipline’ ([44]). With the repeal of the relevant provisions under that Act his suspension was reissued on 9 March 2023 under the Public Service Act. There are two grounds for suspension set out in s 101(1). They are either:
(a) the employee is liable to discipline under a disciplinary law; or
(b) the proper and efficient management of the entity might be prejudiced if the employee is not suspended.
The letter advising him of his continued suspension referred to s 101(1)(b), not s 101(1)(a). It is not explained why the suspension did not refer to 101(1)(a) when that would have been consistent with the reasons given for the original suspension. Commissioner McLennan noted (at [51]) that the Public Sector Act s 104 only allowed for suspension without pay where the suspension was made under s 101(1)(a), not s 101(1)(b). She said (at [52]-[53]):
… while the default position is taken to be ‘suspension with pay’, it is nonetheless open to the chief executive to decide otherwise, only if satisfied of the relevant criteria. The first criterion being that the suspension is under s 101(1)(a) – that is not the case here. The Appellant was notified by QAS on 9 March 2023 that his suspension was pursuant to s 101(1)(b) of the PS Act. There is no need to go on to examine the second criteria set out at section 101(4)(b) because the Appellant’s suspension was not reissued under s 101(1)(a).
Simply put, s 101(4) means that the Appellant is entitled to remain suspended from duty on full remuneration because the suspension notice was reissued pursuant to s 101(1)(b). Section 101(4) provides no capacity to suspend the Appellant without pay in circumstances where his suspension notice was not given under s 101(1)(a).
The respondent ambulance service argued that they were not suspending him without pay. Rather they were lifting his suspension but given his registration was suspended he could not return to work but could draw on any accrued leave. Commissioner McLennan rejected that as it was not consistent with one of the possible outcomes of suspension quoted above. She said (at [57]) ‘… cancelling the paid suspension and ‘inviting’ the Appellant to be paid from his own leave accruals (until those are exhausted presumably, and such payment then stops) is not one of the final outcomes’ permitted under the Act.
As an aside, I would think it is arguable that the decision was a decision where ‘suspension is lifted and the employee returns to normal duties’, but immediately had to take leave as he could not perform those duties. That argument was not expressly considered.
Commissioner McLennan went onto say (at [58]) that even if her analysis was wrong:
… the Respondent’s ability to make a different decision about the terms of the Appellant’s suspension from duty is not an unfettered power. Such decision must be fair and reasonable. It should only be exercised in limited circumstances – and in a way consistent with the mandatory requirements (in particular, natural justice)…
What the respondent was required to do, and did not do, was set out in the legislation. A notice had to include details of appeal rights, had to identify ‘what duties or other options had been identified and considered, including any reason why the employee could not undertake those alternative options’. He had to be given ‘natural justice’ which requires fundamentally that a person be given a reasonable opportunity to make their case to a decision maker and their submissions will be considered before an adverse decision is made (see [63] for a more detailed explanation of the requirements of natural justice].
Guidance for decision makers confirmed the need to invite people to ‘show cause’ and to give at least 7 days for an employee to response to a show cause notice. At [67] Commissioner McLennan said:
I have carefully reviewed the application of natural justice in the Appellant’s case. In my view the Appellant was not afforded natural justice, as there were several deficiencies in the process:
- The Appellant was not afforded procedural fairness, in relation to the cancellation of his suspension on full pay (where the ‘final outcome’ was other than a return to work, resignation or termination of employment).
- The Appellant was not afforded procedural fairness, in relation to a decision to effectively place him on unpaid suspension. He was not invited to show cause as to why the suspension should not be unpaid.
- The QAS correspondence dated 24 March 2023 did not contain information as to the Appellant’s appeal rights.
- The chief executive is required to “provide the employee with a minimum of 7 days from the date of receipt of a show cause notice to consider and respond to the notice”. That is a requirement to hear the Appellant before a decision is made. It is not the same as giving the Appellant 7 days’ notice of the decision to change the terms of the suspension from ‘suspension from duty on full remuneration’.
- The Respondent’s submission that some representations were nonetheless made on the Appellant’s behalf on the evening of Friday 24 March 2023, in response to the QAS correspondence, does not discharge the mandatory requirement to give the Appellant an opportunity to be heard before a decision is made.
- It was not open to the chief executive to decide that the Appellant ought not be suspended from duty on full remuneration because his suspension was not issued under section 101(1)(a) of the PS Act. That is because suspensions issued under s 101(1)(b) may only be on full remuneration, pursuant to s 101(4) of the PS Act.
In considering what was ‘fair and reasonable’ Commissioner McLennan noted (at [76]-[77]) that if the decision were to stand ‘the Appellant would be lurched into dire straits financially and denied the income he relies on for an undefined period’ and this would happen without being given the opportunity to be heard. She also noted (at [78]) that the period of suspension with pay had been significantly shorter, that is it was ‘less favourable treatment than extended’ to two teachers who had also been suspended pending the outcome of similar charges.
The Commissioner reminded us:
People are presumed innocent until the required standard of proof has been discharged to determine otherwise. The proceedings may yet exonerate the Appellant. We do not know.
The Commission determined that the decision was not fair and reasonable and it was set aside.
ConclusionBeing as generous as one can one might infer that the decision makers at QAS were confused by the introduction of new suspension provisions under the Public Sector Act. They further, given them the benefit of the doubt, presumably believed that they were not moving from suspension with pay to suspension without pay but rather from suspension to no suspension save that Mr Roche could not return to work as his registration had been suspended.
Being less generous one might infer that they saw an opportunity, when notified that Mr Roche’s registration had been suspended, to avoid continuing to pay him without having to go through the natural justice process by relying on the decision of the Health Ombudsman to have the effect that they wanted. But, said the Commission, changing his status had to be ‘fair and reasonable’ and this decision was not.
This blog is made possible with generous financial support from the Australasian College of Paramedicine, the Australian Paramedics Association (NSW), Natural Hazards Research Australia, NSW Rural Fire Service Association and the NSW SES Volunteers Association. I am responsible for the content in this post including any errors or omissions. Any opinions expressed are mine, and do not necessarily reflect the opinion or understanding of the donors.
Who is detaining the person – the police or the mental health facility (NSW)
Today’s correspondent continues the discussion about the role of hospital security staff. My correspondent is concerned that:
… nursing staff are receiving handover and taking over patients who are being bought in under schedule (Mental Health Act) schedule 1, section 20 or section 22 though the patient is noted to be in Police custody, we have been told by our management that police can handover a patient in custody if the clinician is willing to accept the patient and we then contact the police back after the patient has been dealt with under the Mental Health Act and/or assessed. We have never had this issue with previous management as Police were always to stay with the section patient who was in custody up and until they were assessed by the hospital psychiatrist and admitted to the mental health unit otherwise the police were to remain with the patient at all times and the patient was not to be handed over to the hospital due to the patient being in custody?
I am asked to ‘please provide some clarification on this above matter’.
My correspondent provided this screen shot of some relevant paperwork:
{kind=link}
Along with these instructions:
The Mental Health Act{kind=link}
The Mental Health Act 1987 (NSW) s 18(1) says:
A person may be detained in a declared mental health facility in the following circumstances–
(a) on a mental health certificate given by a medical practitioner or accredited person (see section 19),
(b) after being brought to the facility by an ambulance officer (see section 20),
(c) after being apprehended by a police officer (see section 22)…
Where my correspondent refers to schedule 1 that is actually a reference to the form that a doctor must complete in order to authorise a person’s detention eg where a GP has examined a patient and forms the view they should be examined by a psychiatrist and detained until that can happen. The question, more accurately, should say ‘… patients who are being bought in under sections 19, 20 or 22 …’.
A person may be having a mental health crisis and be observed by a doctor, an ambulance officer, or a police officer. A doctor may elect to write a certificate whilst an ambulance or police officer may elect to transport the person to a declared mental health facility. Where a doctor has written a certificate, they may endorse the certificate to the effect that police assistance is required (s 19(3)). Ambulance officers may also request police assistance (s 20(2)). Where a doctor or an ambulance officer has requested police assistance, that assistance must be provided (s 21).
It follows that the police can become involved at the request of a doctor or ambulance officer or on their own initiative. Police may become involved if a mentally ill person is or may be committing a crime. The police may be called and form the view that the person may be mentally ill and that it would be better for everyone if they were dealt with as a patient rather than as a criminal.
Law Enforcement (Powers and Responsibilities) Act (LEPRA)Apart from the power to detain under s 22, above, police as law enforcement have the power to arrest as part of the processes of the criminal law. The Law Enforcement (Powers and Responsibilities) Act 2002 (NSW) (LEPRA) s 99(1) says:
A police officer may, without a warrant, arrest a person if–
(a) the police officer suspects on reasonable grounds that the person is committing or has committed an offence, and
(b) the police officer is satisfied that the arrest is reasonably necessary for any one or more of the following reasons–
(i) to stop the person committing or repeating the offence or committing another offence,
(ii) to stop the person fleeing from a police officer or from the location of the offence,
(iii) to enable inquiries to be made to establish the person’s identity if it cannot be readily established or if the police officer suspects on reasonable grounds that identity information provided is false,
(iv) to ensure that the person appears before a court in relation to the offence,
(v) to obtain property in the possession of the person that is connected with the offence,
(vi) to preserve evidence of the offence or prevent the fabrication of evidence,
(vii) to prevent the harassment of, or interference with, any person who may give evidence in relation to the offence,
(viii) to protect the safety or welfare of any person (including the person arrested),
(ix) because of the nature and seriousness of the offence.
Section 105 says:
(1) A police officer may discontinue an arrest at any time.
(2) Without limiting subsection (1), a police officer may discontinue an arrest in any of the following circumstances–
(a) if the arrested person is no longer a suspect or the reason for the arrest no longer exists for any other reason,
(b) if it is more appropriate to deal with the matter in some other manner…
DiscussionIt is the interplay of the powers of arrest and the Mental Health Act that concerns my correspondent.
Let us assume that a police officer is called to a scene where a person who ‘appears to be mentally ill or mentally disturbed’ has engaged in conduct that, on its face, appears to be criminal eg they have damaged someone’s property or injured another person. The police officer may well decide to make an arrest as they have the suspicion required by s 99(1)(a) and they form the view that the arrest is warranted by virtue of ss 99(1)(b)(i), (ii) and (viii).
Having made the arrest and taken the person into custody there is now no immediate threat that the offending will continue, and the victim is no longer at risk. The officer now needs to decide whether to proceed along the criminal route, which would involve things like taking the person back to the police station to be interviewed, considering whether the person can be released either on bail or own their own undertaking and issuing a court attendance notice. The officer may be aware that if the person is indeed mentally ill they may not be criminally responsible for their conduct, and a prosecutor should only proceed if there are reasonable prospects of success so a determination of the person’s mental health status is important. Also, if the person is mentally ill it would be beneficial for them and the community that their underlying health issues are dealt with.
The police officer may then form the view that it would be more appropriate (s 105(2)(b)) to deal with the person under the Mental Health Act, so they proceed to take the person to the declared mental health facility relying on s 22. Given the person may be detained at the mental health facility it is appropriate to terminate the arrest on the grounds set out in s 105(2)(a) and (b)). At that point that the person is being detained by the mental health facility there is no need or authority for police to stay to maintain the person’s custody.
Police can ask, as they do, that if the person is to be discharged that they want to know so they can again revisit the decisions. If the psychiatrist assesses the patient and determines they are not mentally ill or do not meet the criteria for involuntary admission, the police may want to proceed with criminal proceedings.
LEPRA Part 9The discussion above is not inconsistent with the instruction that:
Police are required to maintain a guard on a person within a health facility who is brought there in their custody under Part 9 of LEPRA and who remains in their custody.
Part 9 of LEPRA deals with investigation and questioning. It allows police to detain a person, without charge, whilst certain investigations are complete. Whilst being so detained a person has a right to medical attention (s 129). Section 138 says:
A medical practitioner acting at the request of a police officer of the rank of sergeant or above, and any person acting in good faith in aid of the medical practitioner and under his or her direction, may examine a person in lawful custody for the purpose of obtaining evidence as to the commission of an offence if–
(a) the person in custody has been charged with an offence, and
(b) there are reasonable grounds for believing that an examination of the person may provide evidence as to the commission of the offence.
One can imagine that a prisoner may be brought to the hospital because they require medical attention or the police want an examination to collect evidence eg an x-ray to see if the person has swallowed drug packets, or a blood test etc. It is in those circumstances, where the arrest is continuing and the whole point of the exercise may be the collection of evidence, that it is police who must maintain the custody of the person.
A person who has been brought to a hospital under s 22, even if they had been arrested, is not a person in police ‘custody under Part 9 of LEPRA’.
The view of ‘previous management’What concerns me is the final statement of the original question:
We have never had this issue with previous management as Police were always to stay with the section patient who was in custody up and until they were assessed by the hospital psychiatrist and admitted to the mental health unit otherwise the police were to remain with the patient at all times and the patient was not to be handed over to the hospital due to the patient being in custody?
Why it concerns me is that, reading between the lines, it implies a misunderstanding of what custody means and the role of police and the health facility and that is a worry if that misunderstanding was held, and promoted by ‘previous management’.
A person who is brought in under s 22 is not in police custody. They have been detained for the purpose of taking them to a health facility for care. The police detention ends when the person is delivered to the care of the facility, not on assessment by a psychiatrist. If the person has been arrested that arrest can, and should be, terminated whilst the person is being detained in the health facility for the reasons set out in s 105 of LEPRA.
A person who is brought into a declared mental health facility by police acting under s 22 can be detained at the facility for up to 12 hours (Mental Health Act 2007 (NSW) s 27(1)(a)). If there is a secured mental health ward the person could be located there without first being seen by a psychiatrist, that is the whole point of ss 19 and 22. The person can be detained on the basis of the information provided by police alone. It would be a waste of police and community resources to take police away from their other duties for up to 12 hours when a declared mental health facility should have the facilities to detain people.
Using police to secure the mentally ill is anti-therapeutic. At that time the person is in the care of a health facility for assessment and if necessary, treatment and care. Having uniformed and armed police in the ward would not be good for anyone. Being able to care for people in a secure environment should be part of the core business of a declared mental health facility.
ConclusionIn my view it is not only lawful it is entirely appropriate that ‘police can handover a patient in custody if the clinician is willing to accept the patient and we then contact the police back after the patient has been dealt with under the Mental Health Act’. Such action is consistent with both the Mental Health Act and LEPRA.
This blog is made possible with generous financial support from the Australasian College of Paramedicine, the Australian Paramedics Association (NSW), Natural Hazards Research Australia, NSW Rural Fire Service Association and the NSW SES Volunteers Association. I am responsible for the content in this post including any errors or omissions. Any opinions expressed are mine, and do not necessarily reflect the opinion or understanding of the donors.
Dismissed paramedic loses further appeal
Sally-Anne John, a NSW paramedic who uploaded video of her attendance, and intemperate rant against police, at a COVID-19 protest lockdown was originally suspended by the Paramedicine Council (see NSW Paramedic suspended after participation in COVID-19 protests (April 14, 2023)) and then her employment was terminated by NSW Ambulance. She made an unsuccessful application for a remedy under the unfair dismissal laws – see Protesting paramedic’s dismissal confirmed (July 30, 2023). She has returned to the Industrial Relations Commission to appeal against the decision of the Commission to refuse to order NSW Ambulance to reinstate her employment – John v Health Secretary in respect of Ambulance Service of NSW (No 2) [2023] NSWIRComm 1115 (30 November 2023) (Chief Commissioner Constant, Commissioner Muir and Commissioner McDonald). Once again she has been unsuccessful.
Ms John sought to tender further evidence. An appeal is not a chance to run the case again, it is a place to argue that a mistake was made by the ‘lower’ tribunal. It is unusual for appeal tribunal to receive new evidence and they must give permission to do so. The Full Bench can, however, receive fresh evidence (at [22]) if ‘… there are compelling and exceptional reasons why evidence which was available at the time of the hearing was not adduced…’.
The evidence she wanted to bring in was her medical file from her GP pratice. At the first hearing she had tendered two letters from treating doctors, one of which was admitted into evidence and one was not. Now she wanted to tender the whole file. She argued (at [11]) that
The medical evidence establishes that Effexor withdrawal can lead to a range of severe and prolonged symptoms, including but not limited to mood swings, aggression, and impaired decision-making. These symptoms often persist for an extended period beyond the cessation of the medication. The evidence demonstrates a strong correlation between the onset of these symptoms and my alleged misconduct.
She also wanted to rely on some published papers and material from a website, but she failed to provide copies of that material to the respondent ambulance service.
The Commission refused to accept the further evidence. First it had all been available to her at the time of her first application ([44]). At [45]-[46] the Commission said:
The appellant’s explanation as to why she did not obtain and tender the evidence during the initial hearing was that she thought the doctor’s letters she tendered during the proceedings before Commissioner Sloan would have been sufficient to establish her case. Having not succeeded on that basis, she had made efforts to obtain more and better evidence in preparation for this appeal.
It is unfortunate that, as a self-represented litigant, the appellant may have misunderstood the evidence needed to prevail in her application, but this alone is not a basis to permit further evidence on appeal. To allow the receipt of further evidence on this basis would effectively permit the appellant to re-run her case on appeal. As s 191(3) of the IR Act makes clear, the Full Bench cannot substitute its own decision on the matter, but must only intervene if it finds error in the decision below. An appeal to the Full Bench is not a hearing de novo. An appeal does not mean that the primary decision is laid to one side in order to provide the appellate with an opportunity to lead ‘better’ evidence than what was lead previously, in the hope that a different outcome will occur.
As for her evidence as to the effect of her drugs, Ms John wanted to draw conclusions from the scientific papers without putting the papers themselves before the court. At [47] the Commission said:
The appellant did not establish that she has specialised knowledge within the meaning of s 79 of the Evidence Act such as to permit her statements as to the effects of depression and of withdrawal from Effexor to be admitted as evidence to prove those effects. Reference to scientific papers or articles does not cure this difficulty, particularly where copies of the papers and articles were not provided and the appellant was in any event not qualified to interpret and explain them.
In short (at [50]):
It is apparent to the Full Bench … that the appellant seeks to re-run the same case as she ran at first instance, but with more detailed evidence. That is not a basis to receive further evidence.
Having dismissed the application to lead further evidence the Full Bench then had to decide whether Ms John should be given leave (ie permission) to appeal. (In some jurisdictions an appeal is a ‘right’, in others the intending appellant needs ‘leave’). It is very hard to get ‘leave’ if the application is simply that the judge below came to a view of the facts that the appellant disagrees with. Ms John’s appeal was based on the claim that the failure by Commissioner Sloan at first instance was a denial of procedural fairness ([55]) and that if he had received the letter he would have come to a different conclusion.
The full bench noted that Commissioner Sloan had pointed to problems in the letter and said if she wanted to rely on it, the doctor would have to give evidence and be subject to cross examination ([60]) which did not happen. Ms John made no argument that the decision of Commissioner Sloan was a legal error. At [64] the Full Bench said:
As with the appellant’s application to introduce further evidence, the appeal is an attempt to re-run the same case as she ran at first instance, but in this case before a differently constituted Commission. That is clearly not the function of an appeal …
ConclusionMs John put her case for an unfair dismissal remedy but lost. Having got the Commission’s reasons and having seen how the Commissioner dealt with the evidence she lodged an appeal to have another go. Litigation is however, a one-shot process. You put your best case forward. You do not get to run your case at trial and if you lose rely on that as a practice run and then have another go in the appeal courts. The decision to dismiss Ms John from NSW Ambulance stands.
This blog is made possible with generous financial support from the Australasian College of Paramedicine, the Australian Paramedics Association (NSW), Natural Hazards Research Australia, NSW Rural Fire Service Association and the NSW SES Volunteers Association. I am responsible for the content in this post including any errors or omissions. Any opinions expressed are mine, and do not necessarily reflect the opinion or understanding of the donors.
Doctor cannot require security to detain a competent adult – Part 2
After publishing Doctor cannot require security to detain a competent adult (December 2, 2023) I received the following related question:
I work at a major Sydney Hospital (NSW Health) as a Security Officer we are currently being advised by our management team and executives that if we are instructed by a Doctor, nurse or paramedic to Restrain or Detain a patient as a “Duty of care” even if the patient is not scheduled under the mental health act and also has full capacity that we are still to follow the clinicians directions? Can you please provide some information on the above question and also if you are aware of any Security officers which have been terminated or sued civilly??
Am I ware of any Security officers which have been terminated or sued civilly?? Not in the circumstances you describe but in the case discussed in the post No power to detain a patient just because it’s good for them (January 22, 2023) the patient was acquitted of causing grievous bodily harm after the security guards ankle was fractured.
Addressing jury members before they retired to consider their verdict, Judge Black said the man was entitled to leave.
“He was unlawfully brought back into the hospital, and after force was unlawfully applied to him, he was then unlawfully detained and put onto a stretcher, and kept in hospital overnight.”
Judge Black said nobody was suggesting the hospital staff acted with malice, and “no-one was deliberately trying to breach the accused man’s rights”.
But to reinforce her main point, she said, “the law is that he should have been allowed to leave”.
“No one was allowed to touch him.”
It should not need to be restated (but clearly it does; and that’s a reflection on the ‘management team and executives’, not my correspondent) that a patient cannot be detained just because its good for them. There is no duty to protect people from their own choices (Stuart v Kirkland-Veenstra [2009] HCA 15). Anyone who thinks paramedics, nurses or doctors can instruct anyone ‘to Restrain or Detain a patient as a “Duty of care” even if the patient is not scheduled under the mental health act and also has full capacity’ has failed bioethics 101. If anyone thinks they can detain someone because the person should have treatment or examination has missed the point of consent in medical care.
Some law references say:
- The fundamental principle, plain and incontestable, is that every person’s body is inviolate (Collins v Wilcock [1984] 3 All ER 374).
- … all medical treatment is preceded by the patient’s choice to undergo it (Rogers v Whitaker [1992] HCA 58)
- Personal autonomy is a value that informs much of the common law. It is a value that is reflected in the law of negligence. The co-existence of a knowledge of a risk of harm and power to avert or minimise that harm does not, without more, give rise to a duty of care at common law… (Stuart v Kirkland-Veenstra [2009] HCA 15)
- There can be no duty to act in a particular way unless there is authority to do so. Power is therefore a necessary condition of liability… (Stuart v Kirkland-Veenstra [2009] HCA 15).
In other words, a duty of care to act can only arise if there is authority. It is not a source of authority. In Stuart’s case police failed to detain Mr Veenstra who then took his own life. The High Court in a unanimous decision said there was no breach of duty to Mr Veenstra as there was no power, and so no duty to detain him.
A ‘a Doctor, nurse or paramedic’ cannot have a duty to restrain or detain a person who ‘is not scheduled under the mental health act and also has full capacity’. If that person wants to leave, they can go. For further discussion see:
- Transporting sedated patients in WA (December 30, 2019);
- Relying on the concept of ‘duty of care’ to impose treatment on the unwilling (September 30, 2020);
- No power to detain a patient just because it’s good for them (January 22, 2023);
- “Medical law expert issues warning to WA hospital staff over patients who want to leave” (June 22, 2023);
- Publication on detaining patients in the ED (August 29, 2023); and
- What should ‘hospital security staff … get their head around’? (October 26, 2023).
This blog is made possible with generous financial support from the Australasian College of Paramedicine, the Australian Paramedics Association (NSW), Natural Hazards Research Australia, NSW Rural Fire Service Association and the NSW SES Volunteers Association. I am responsible for the content in this post including any errors or omissions. Any opinions expressed are mine, and do not necessarily reflect the opinion or understanding of the donors.
CFA refused access to fire site in FRV fire district
Today’s question is about the right of members of Victoria’s Country Fire Authority (the CFA) at access a significant local industry. I won’t name the industrial site, but one can imagine it is a large, complex secured site. In response to a fire call:
… dedicated Country Fire Authority (CFA) volunteers were shockingly denied access … by on-site service personnel. The denial was allegedly based on the volunteers’ status as non-Fire Rescue Victoria (FRV) members, relegating them to a second-class citizen status.
These CFA volunteers, despite being highly trained and capable professionals, were unjustly hindered from contributing to critical tasks within the major … facility. The denial of their access raises serious concerns about the safety of the community and the employees located within the facility. particularly given their expertise in handling structure fires and years of dedicated response into the [facility] …
This incident not only undermines the dedication and commitment of these firefighters but also jeopardises the safety and well-being of the communities they serve. This matter and that such discrimination against CFA volunteers should be made public to the communities effected by such actions.
It’s not my job to rung public information campaigns or to editorialise on the alleged conduct. My job is to comment on the law, in this case the Country Fire Authority Act 1958 (Vic) and the Fire Rescue Victoria Act 1958 (Vic).
I have confirmed that the site in question is with a Fire Rescue Victoria fire district but, I am told the nearest fire appliance is a CFA appliance and there can sometimes be a 4-5min difference between the arrival of [the CFA] … and FRV’.
The CFA is responsible for the provision of fire services in country Victoria (s 20). To do that officers of the CFA are given the necessary powers to respond to an emergency. In particular s 30(1) says, emphasis added:
Where the Chief Officer believes on reasonable grounds that there is danger of fire occurring or where a fire is burning or has recently been extinguished anywhere within the country area of Victoria the Chief Officer for the purpose of preventing the occurrence of a fire, of extinguishing or restricting the spread of the fire or of protecting life or property shall have and may exercise the following powers and authorities:…
(c) He shall have authority either alone or with others under his command to enter upon any land house building or premises and if necessary to force open any outer or inner doors of any house or building which may be on fire or in the near neighbourhood of any fire for the purpose of taking any steps which he deems necessary for any of the purposes aforesaid, and he may take or give directions for taking any apparatus required to be used at a fire into through or upon any land house building or premises which he considers convenient for the purpose;
(d) He may take any measures which in the circumstances are reasonable and which appear to him to be necessary or expedient for any of the purposes aforesaid and in particular he may cause any house building or structure to be entered into and taken possession of or pulled down or otherwise destroyed or removed, and any fences to be pulled down or otherwise destroyed or removed, and any undergrowth trees scrub grass stubble weeds or other vegetation to be burnt or otherwise destroyed or removed;…
(g) If a person is interfering, by his or her presence or otherwise, with the operations of any brigade or group of brigades or is in or on any land, building or premises that is burning or threatened by fire, the Chief Officer may—
(i) order the person to withdraw and may include in the order a direction to immediately leave any area affected by the fire by the safest and shortest route; and
(ii) in the event that the person fails or refuses to withdraw—remove the person or direct a member of a fire brigade or a police officer present at the fire to remove the person;…
(i) The Chief Officer may take such other measures as appear necessary for the protection of life and property.
The Chief Officer can delegate these powers ‘to any person by name or to the holder of an office or position approved by the Authority’ (s 28). That is, the Chief Officer may (and I infer has) delegated these powers to relevant officer holders eg the captains of local CFA brigades.
It follows that if this industrial site was in country Victoria, the officer in charge of the CFA response, assuming that he or she held the Chief Officer’s delegation could direct the ‘on-site service personnel’ to ‘withdraw’ and direct members of the fire brigade or the police to remove them and the CFA could enter the site, with force if necessary, to perform their fire control functions. But this site was within a FRV fire district?
The Country Fire Authority Act s 2(1) says:
It is the intention of the Parliament that the Country Fire Authority and Fire Rescue Victoria establish processes that will ensure that they—
(a) promote collaboration and coordination between fire services agencies to best meet the safety needs of the community; andrecognise the importance of maintaining capacity to respond to peaks in demand for fire services within fire services agencies; and
(b) recognise and value the contribution of volunteer brigades; and
(c) recognise that both volunteer firefighters and career firefighters are vital to delivering safe and sustainable fire services; and
(d) maintain the ability of fire services agencies to respond to critical incidents, to prevent and suppress fires and to protect life and property.
An identical clause appears in the Fire Rescue Victoria Act (s 2A). The CFA Act also says (s 20AC) that:
… Fire Rescue Victoria must, subject to operational requirements, request the assistance of all volunteer brigades located in the Fire Rescue Victoria fire district for the purposes of endeavouring to—
(a) prevent or suppress a fire in the Fire Rescue Victoria fire district (including preventing a fire spreading to the Fire Rescue Victoria fire district from outside the Fire Rescue Victoria fire district); or
(b) protect life or property in the Fire Rescue Victoria fire district.
Section 93B provides that the CFA may provide firefighting services outside the country area of Victoria when it is requested to do so. These provisions make explicit the expectation that FRV and CFA will work together, and we can infer that is being done when the CFA are responded to this industrial site.
Consistent with these provisions is s 33(2)(c) which says
The powers and authorities conferred by this Act on the Chief Officer in respect of any district are exercisable as follows:…
(c) If there is danger of fire occurring or a fire is burning … at a place in any part of the Fire Rescue Victoria fire district … by the Chief Officer or any officer in charge of any brigade or brigades who is present at that place.
It follows that the officer in charge of the CFA brigade can exercise those powers listed under s 30 and could force entry into the premises. Of course just because one has, in theory, the legal power does not mean one should, one has to consider the risk to those involved in the use of force. Firefighters do not presumably volunteer to get into physical fights with security staff so alternatives to force need to be considered.
DiscussionThe intention of the legislation is that there will be a seamless fire service so that if a person calls triple zero – or a fire alarm is triggered – regardless of where in Victoria a fire service will attend and whether that’s FRV or the CFA should not matter. I imagine both police and FRV would expect that an estate owner would not need to be forced to let the CFA in to do their job.
Giving a large industrial site will have (and does have) its own emergency management team and procedures, the appropriate response may be to raise the issue with FRV and the onsite emergency management team to resolve the instructions that are being given to security and other staff. This may be more effective than a ‘name and shame campaign’ particularly if it turns out the decisions was that of a misguided security officer rather than a corporate policy.
POSTSCRIPT 1When I was first working on this answer I thought I found a section that said the CFA could exercise their s 30 powers in a FRV fire district in the absence of anyone from FRV. A provision to that effect is in place for FRV (see Fire Rescue Victoria Act s 55E(4)), but after working in it – for hours – today I could not find it so I assume I just imagined it. But if anyone is aware of a section I’ve missed, do please let me know.
POSTSCRIPT 2After writing the above, and a different conclusion, tiggerific2014 wrote a comment pointing me to s 33(2)(c) and confirming that I indeed did not imagine it. I have updated the post accordingly.
This blog is made possible with generous financial support from the Australasian College of Paramedicine, the Australian Paramedics Association (NSW), Natural Hazards Research Australia, NSW Rural Fire Service Association and the NSW SES Volunteers Association. I am responsible for the content in this post including any errors or omissions. Any opinions expressed are mine, and do not necessarily reflect the opinion or understanding of the donors.
Doctor cannot require security to detain a competent adult
Today’s correspondent is a:
… security officer in a major Sydney hospital [who] would like [my thoughts] … on an issue we are facing. We have a patient who is an adult and was declared by the hospital doctor to have capacity, was not scheduled and parents wanted to take him home.
The doctor demanded that security physically stop him from leaving as we are to comply with a lawful medical direction. My question is am I liable to prosecution as I believe this was not a lawful demand and can I be sued in civil court.
It’s a shame that it must be constantly stated – a competent adult can refuse medical care at any time and for any reason. The test is competence not wisdom. It may be a bad decision, but it is their decision.
Of course I have no idea why the doctor wants the person stopped and there may be more complex issues but taking the story on its face.
As an employee you are obligated to obey the reasonable directions of your employer. The doctor is not your employer. A doctor doesn’t have the right to detain a mentally competent adult and cannot authorise anyone else to do so. Even if it was part of your duties to ‘comply with a lawful medical direction’ a direction to physically stop a mentally competent adult from leaving a health facility would not be a ‘lawful’ direction.
Could you be liable to prosecution for restraining the patient? Yes indeed. An honest belief in facts that if true would make the act innocent is a defence – so an honest belief that the patient was not competent may be a defence, but you do not hold that belief. A belief that the doctor had the authority to issue the direction would be a mistake of law, not of fact. Mistake of law is no defence so even if you thought the doctor’s direction was a lawful authorisation that would not be a defence.
Can you be sued? Again, the answer is yes but here that is unlikely. The patient, if they wanted to sue anyone, would sue the hospital as they would have the funds to pay the damages and they are responsible for your training and the doctor’s training. If there was a failure to protect the patient the failure is the hospital’s failure.
See also:
- No power to detain a patient just because it’s good for them (January 22, 2023);
- “Medical law expert issues warning to WA hospital staff over patients who want to leave” (June 22, 2023);
- Publication on detaining patients in the ED (August 29, 2023); and
- What should ‘hospital security staff … get their head around’? (October 26, 2023).
This blog is made possible with generous financial support from the Australasian College of Paramedicine, the Australian Paramedics Association (NSW), Natural Hazards Research Australia, NSW Rural Fire Service Association and the NSW SES Volunteers Association. I am responsible for the content in this post including any errors or omissions. Any opinions expressed are mine, and do not necessarily reflect the opinion or understanding of the donors.
Today’s industrial action by Australian Paramedics Association prohibited by the Industrial Relations Commission
The Australian Paramedics Association (the APA) has been conducting an extensive campaign to fit for better wages and conditions for NSW Ambulance Paramedics. As part of the campaign they had proposed to impose industrial bans between 7am and 7pm today, 1 December 2023. During that time APA members would only respond to Priority 1 (1A, 1B and IC) calls.
The Health Secretary sought orders from the Industrial Relations Commission to prohibit the action on the basis that ‘the proposed industrial action constitutes a risk to the health and safety of the public, as well as having flow-on impact on other health entities and emergency services’ – Health Secretary in respect of NSW Ambulance v Australian Paramedics Association (NSW) [2023] NSWIRComm 1116 (30 November 2023) (Commissioner Webster), [1]).
During conciliation (that is an attempt to bring the parties to agreement) the Commission recommended and the APA accepted that they would respond to ‘category 1 a, b and c, 2 (i) and R4 service calls’ ([3]). The Commission recommended but that APA rejected that the industrial action be limited to one hour. The APA intended to proceed with the 12 hour stoppage ([3]).
The matter then proceeded to arbitration where the Commission could make binding orders. Evidence was led by the Ambulance Service as to the number of patients that may be affected and the potential implications for the health service generally. The APA led evidence as to steps that could be taken, and that APA would cooperate with, in order to minimise the impact eg ‘additional people to monitor the jobs not being attended to’ ([12]). At [15] Commissioner Webster said:
I accept the evidence of Mr Simpson that there are available to the service mitigation strategies to reduce the impact of the industrial action on the public. Further, it is important to that his evidence with respect to the notice given the service and the offers of assistance from the APA were not contested.
The Commission acknowledged the passion and frustration evident in the testimony of the APA witnesses ([31]) but could not accept either that there was no greater risk to patient safety because the health care system already put patients at risk ([26]) or that the action would enhance public safety by increasing the availability of ambulances to respond to priority 1 calls. Commissioner Webster said (at [29]):
… the APA stated that the impact of patients was acknowledged … That is to say, they know they will be letting down patients, but the bigger picture reason for the industrial action of improving the Service in the long term justifies it. I do not agree. I am concerned that vulnerable people in the community will be significantly impacted by the industrial action. This is an unacceptable consequence of the industrial fall out between the parties.
Finally at [33] the Commissioner said:
The Ambulance Service is an important essential service for the community of NSW. It is not a service that the community can be without for a single day. I acknowledge the APA has designed the scope of the proposed industrial action to ensure that patients experiencing the highest acuity will not be impacted. However, I am also concerned that the industrial action is likely to have an impact on highly vulnerable members of our community, including the elderly… There is a strong public interest in ensuring the health and welfare of people seeking to access the Ambulance Service.
The Commission made orders directing the APA to call off the industrial action that had been scheduled for today. The orders banning the action remain in force until 11 January 2024 ‘six-weeks from now. In [Commissioner Webster’s] view this is long enough for the parties to consider their respective positions and plan for ongoing negotiations’ ([34]).
It should be noted that the other ambulance union, the Health Services Union, is running a campaign asking paramedics not to renew their registration – see Potential consequences of proposed NSW Ambulance industrial action (September 16, 2023). This case had nothing to do with that action.
This blog is made possible with generous financial support from the Australasian College of Paramedicine, the Australian Paramedics Association (NSW), Natural Hazards Research Australia, NSW Rural Fire Service Association and the NSW SES Volunteers Association. I am responsible for the content in this post including any errors or omissions. Any opinions expressed are mine, and do not necessarily reflect the opinion or understanding of the donors.
NSW Ambulance and GoodSAM App
I have previously written about the GoodSAM App that dispatches willing volunteers to ambulance calls to encourage early CPR where that is required – see
- Crowd sourcing first aid (August 12, 2014);
- Responding third parties to 000 ambulance calls (May 7, 2023); and
- The GoodSAM App and good Sam(aritan) laws in Queensland (October 27, 2023).
NSW Ambulance have announced that they have now joined up with GoodSAM and can respond volunteers to cases where CPR may be required – see NSW Ambulance GoodSAM (undated).
I have two concerns with the NSW Ambulance announcement. First on the page Volunteering with GoodSAM, they say:
You can become an GoodSAM volunteer if you are:
- 18 or over
- willing and able to perform CPR. Formal First aid or CPR training are not necessary.
Not requiring a volunteer to at least have some training is creating a risk of adding a number of bystanders with no skill to an already hectic situation. Presumably there is already at least one person on the scene, it the person calling triple zero. Adding more people who may have watched a video but have no more experience is sending a lot of people to the scene who may or may not be able to add anything and who may just want to watch.
The page Responding as a GoodSAM volunteer says:
If the scene is safe, introduce yourself to any bystanders or family members as a GoodSAM responder. Explain that NSW Ambulance has told you that someone needs help, and that an ambulance is also on its way…
Once you have introduced yourself, perform CPR or use an AED.
I think people would expect that someone responding does have some training and they are going to let the volunteer act on that basis. Without training they’re just another bystander although I accept that they contribute a lot if they have managed to collect an AED along the way and they may also make an invaluable contribution if they are the only other bystander on scene.
When I first saw this App as it was operated in WA a person had to upload a current first aid certificate to be registered as a responder. It probably doesn’t affect the legal issues but it does seem to me that it would be reasonable to limit volunteers to those who have demonstrated some competence in the skill they are being asked to perform – both for the protection of the responder and the potential patient and other bystanders.
My other concern is really just a typo. On the page ‘Staying Safe’ it says
… As a GoodSAM responder, you are covered by NSW Ambulance’s personal accident and injury insurance, as well as medical indemnity insurance.
Giving Chest Compressions to a nearby person after a GoodSAM alert is the same as if you’d seen them collapse yourself. As a member of the public providing simple first aid, you are protected as a Good Samaritan under the Public Liability Act 2002 (NSW).
The typo is that there is no Public Liability Act 2002 (NSW). They mean the Civil Liability Act 2002 (NSW).
The statement ‘… As a GoodSAM responder, you are covered by NSW Ambulance’s personal accident and injury insurance, as well as medical indemnity insurance’ is very generous. In my post Responding third parties to 000 ambulance calls (May 7, 2023) I argued that the use of the GoodSAM app by NSW Ambulance could mean that a volunteer was eligible for compensation under the Workers Compensation (Bush fire, Emergency and Rescue Services) Act 1987 (NSW) or as deemed employees of NSW Ambulance. It certainly seems that NSW Ambulance is willing to accept that sort of liability. It does create an anomaly that a bystander at the scene who suffers an injury whilst doing CPR would get nothing, but a bystander who goes to the scene in response to a GoodSAM app may get compensation for the same injury even though the cause of injury and motivation is the same.
This blog is made possible with generous financial support from the Australasian College of Paramedicine, the Australian Paramedics Association (NSW), Natural Hazards Research Australia, NSW Rural Fire Service Association and the NSW SES Volunteers Association. I am responsible for the content in this post including any errors or omissions. Any opinions expressed are mine, and do not necessarily reflect the opinion or understanding of the donors.
Vicarious liability for volunteers
Throughout this blog I have talked about vicarious liability – the rule that an employer is labile if their employee is negligent even where the employer has not been negligent in the way they select or manage employees. I have also argued that agencies that use volunteers – in this context the emergency services – will also be vicariously liable for the negligence of their volunteers even though there is no employer/employee relationship.
Bishop Paul Bernard Bird v DPThat argument has been tested albeit in contexts removed from the emergency services. In the first case, Bishop Paul Bernard Bird v DP (a pseudonym) [2023] VSCA 66, the Victorian Supreme Court of Appeal had to determine whether the Diocese of Ballarat (the ‘Diocese’) through the current Bishop, Paul Bird, was vicariously liable to DP for historic sexual abuse by one of the church’s assistant priests, Father Bryan Coffey. Coffey was neither an employee nor an independent contractor ([77]).
The applicant argued that vicarious liability can only apply where there is an employment relationship. The Court of Appeal rejected this holding (at [82]) that, after a review of the legal precedents:
… it is evident that the principle of vicarious liability has not been confined solely and exclusively to cases in which the relationship between the tortfeasor and the principal is that of employer and employee. In particular, it has been recognised in the authorities that, in certain circumstances, vicarious liability may apply in respect of a relationship which is not that of employment.
A significant case in this area is Hollis v Vabu (2001) 207 CLR 21 where the High Court determined that a courier company was vicariously liable for the negligence of the courier. In that case the High Court found that the company was an employer even though it had tried to structure the arrangements to ensure the couriers were independent contractors. Even so the Court of Appeal in DP’s case said (at [94]):
… the decision in Hollis is important, because it demonstrates the relevance and significance, as a criterion of vicarious liability, of the circumstance that the particular tortfeasor’s role was so closely tied with the enterprise of the employer that he or she was presented to the public as carrying out the work of, and representing, the employer.
Important factors identified by the majority (Gleeson CJ, Gaudron, Gummow, Kirby and Hayne JJ), and McHugh J in a separate judgement were:
… the right of the principal to control the work performed by the agent, and the circumstance that the agent was working in, and for the economic benefit of, the business of the principal.
In Sweeney v Boylan Nominees Pty Ltd (2006) 226 CLR 161 the defendant was not vicariously liable for the conduct of a fridge mechanic that failed to properly fix a commercial fridge so that the door fell onto a customer. In that case (at [103]):
… the defendant did not control the way in which the mechanic worked, the mechanic supplied his own tools and equipment, and brought his own skills to bear on the work that was done, and that, unlike in Hollis, the mechanic ‘was not presented to the public as an emanation of the respondent’.
At [114]-[116] the Court of Appeal said:
… a relationship may give rise to vicarious liability on the part of a principal, notwithstanding the tortfeasor [wrongdoer] was not an employee of the principal. In such a case, vicarious liability is imposed on the principal for the actions of the tortfeasor, on the basis that the work performed by the tortfeasor and the business of the principal were so interconnected that the tortfeasor represented the business of and/or the principal, and, by doing so, conducted the business of the principal…
… central to the application of the principle to employees is that, inherent in the relationship, is a contractual right of the employer to control the performance of the duties of the employee. By being subject to such control, the employee necessarily forms part of or represents the enterprise of the employer…
The Court then went onto consider ‘whether, applying the principles which we have discussed’ the evidence demonstrated relationship between the Diocese and Coffey, that would attract vicarious liability even though Coffey was not an employee. Finding that a relevant relationship did exist the court noted (at [124]-[129]) that:
- Coffey was appointed to his role by the Bishop;
- The relationship was governed ‘by a strict set of normative rules that each of them had subscribed to… Those rules of Canon law also permitted the Bishop to exercise control over Coffey that was at least as great as, if not greater than, that enjoyed by an employer…’;
- The Bishop could exercise control over Coffey ‘… by providing instruction, supervision, transfer, limitation on authority, and ultimately by seeking sanctions, including expulsion, from church authority. In return the priest was clothed with the authority of the church.’
- … in his work as assistant priest, Coffey was very much a representative, and conducted the work, of the Diocese. His role, and the work he performed in undertaking that role, was necessarily and integrally interconnected with the fundamental work and function of the Diocese. In discharging his duties in that role, Coffey was not acting independently of the Diocese, but as a representative of it.’
- He wore the uniform of a priest.
- ‘As assistant priest, duly appointed by the Bishop, Coffey did the work of the Diocese … and the Diocese did its work by and through him. In a real and relevant sense, Coffey was the servant of the Diocese, notwithstanding that he was not, in a strict legal sense, an employee of it.’
The issue next arose in Kneale v Footscray Football Club Ltd [2023] VSC 679. In this case Richards J held that the football club was not vicariously liable for the wrongful conduct of a volunteer – the wrongful conduct again being historic sexual abuse. Her Honour considered the role of the wrongdoer in this case was unlike the role of the priest. She said (at [36]-[37]):
… the relationship between the Club and Hobbs in this case did not remotely resemble that between the Diocese and the assistant priest in Bird. I note in particular the following:
(a) Hobbs’ roles with the Club were informal, undocumented, and uncertain. The Club had no written policies regarding the recruitment, supervision, or control of its volunteers. This informality contrasts with the ‘strict set of normative rules’ that enabled the assistant priest to embody the Diocese in Bird.
(b) The work performed by Hobbs was to sell membership and raffle tickets to the public, along with other volunteers. Hobbs also claimed to have looked after the office when no-one was there and to have been a ‘doorman type thing’. No‑one was quite sure what work he did for the Under 19s team. Although he was well known and a constant presence at the Club, it was not possible to say that the work he performed was so interconnected with the business of the Club that he was, in effect, conducting that business.
(c) Although the handling of money by volunteers was supervised, there was no evidence that the Club exercised control over Hobbs in relation to any other aspect of his work. … The supervision of Hobbs’ work with the Under 19s was so slight that no-one could say what work he in fact did.
(d) While there was a good deal of evidence that Hobbs exploited his access to Club premises and membership tickets, there was no evidence that the Club clothed him with authority to represent it in anything other than selling tickets and raising funds.
(e) There was no evidence that Hobbs wore a uniform or any garments associated with the Club. While most of the Under 19s personnel in the group photo in the June 1987 edition of The Bulldog wore some kind of uniform, Hobbs did not.
For those reasons, I did not consider that there was evidence on which the jury could reasonably have found that the relationship between the Club and Hobbs was one in which vicarious liability could arise.
Emergency servicesThese cases are not about the emergency services but are about when there may be vicarious liability even when there is no employment. The question is to ask whether a volunteer in the emergency services looks more like the priest Coffey, or the sports volunteer Hobbs.
Members of the emergency services are generally appointed by the Chief Officer, there are strict rules and procedures in place including requirements for training, the exercise of delegated authority by people who complete relevant training and obtain various ranks, there are detailed and formal procedures to impose sanctions up to and including dismissal. An emergency service has prescribed functions and duties but it cannot perform them without its volunteers. The volunteers represent their service as shown by their uniforms and the vehicles. The work they perform is ‘necessarily and integrally interconnected with the fundamental work and function’ of the service to which they volunteer. They do the work of the service.
Even if members may provide some of their own equipment (eg a pocket knife or a belt pouch) emergency service members are issued with the principal tools necessary to do their work – their uniforms and other PPE, vehicles, fire fighting equipment, flood boats, life jackets, rescue cutting tools, first aid kits, defibrillators etc.
They cannot delegate their tasks other than in accordance with the rules of their organisation. If a person engages with a business as an independent contractor, they get a task but it is then up to them to decide how the task is done, and they may do it themselves or get their own staff to do it. Consider for example if you engage a plumber – you tell them the problem and they work out how to fix it and they may do it themselves or get their apprentice, who you’ve never met to do it. In the emergency services a unit commander may be tasked to do something and he or she can delegate to members in the unit but they cannot delegate the task to someone outside the organisation. How they perform the task, and to whom they can assign roles are all determined by the organisation.
Unlike the priest, emergency service volunteers do not earn their livelihood from the work nor is it necessarily their ‘full time’ engagement. But unlike Hobbs, their work is not ‘informal, undocumented, and uncertain’. Emergency service volunteers are controlled through the chain of command, codes of conduct and in most cases legislation.
ConclusionI would suggest the amount of control and the integration of emergency service volunteers into the work of the emergency services organisation looks much more like Coffey than Hobbs. In those circumstances I am confirmed in my view that an emergency service organisation will be vicariously liable for the torts of its volunteers even though they are not employees.
This blog is made possible with generous financial support from the Australasian College of Paramedicine, the Australian Paramedics Association (NSW), Natural Hazards Research Australia, NSW Rural Fire Service Association and the NSW SES Volunteers Association. I am responsible for the content in this post including any errors or omissions. Any opinions expressed are mine, and do not necessarily reflect the opinion or understanding of the donors.
Thank you for your service
Already this summer reminds us of how dangerous emergency service work can be. Australian Emergency Law recognises and honours the sacrifice made by so many so early in the season – two NSW RFS firefighters – a volunteer firefighter who died after being struck by a falling tree near Walgett yesterday, and Senior Deputy Captain John Holmes who died while fighting a blaze at Bean Creek near Kyogle on October 14; and the three aircrew who died while engaged in fire surveillance in remote north-west Queensland, on 4 November. I also pay my respects to Western Australia paramedic Tinesh Tamilkodi who died on Tuesday whilst proceeding to an emergency call.
Their sacrifice and the loss to their families gives us all reason to pause and reflect on the work done by so many to protect our communities and to respond to other people’s emergencies and to thank everyone involved for their service.
{kind=link}
{kind=link}
{kind=link}
Using the term ‘ambulance’ in WA
Today’s question is
I live in Western Australia and lately we have seen an explosion in private ambulance companies.
When I was at a school event I noticed a vehicle there providing first aid however it wasn’t your Traditional Mercedes Sprinter Van ambulance. It was a small SUV with the word ambulance. And it also had a light bar on the top. My question is, is there any regulation around who is allowed to put the word ambulance and have light bars on their vehicles because it appears that there are so many private companies that don’t respond to emergencies but have the word ambulance on their vehicles.
In WA there is no law that says who can or cannot put the word ‘ambulance’ on their vehicles or operate an ambulance service.
With respect to flashing lights, the Road Traffic (Vehicles) Regulations 2014 (WA) r 327(2)(a) says ‘unless subregulation (3) applies, a vehicle must not display — (a) a light that flashes…’ Sub-regulation 3 says ‘an exempt vehicle may be fitted with any light or reflector approved by the CEO’. An exempt vehicle includes an ‘emergency vehicle’ (r 327(4)). Relevantly the term emergency vehicle includes an ‘ambulance’, but that term is not further defined (r 226).
It follows that anyone in Western Australia can put the word ‘ambulance’ on their vehicle and if the Department of Transport accepts that a vehicle is an ‘ambulance’ then it can have any light, including a flashing light, that the CEO has approved for fitting to emergency vehicles which, presumably, includes red/blue flashing lights.
This blog is made possible with generous financial support from the Australasian College of Paramedicine, the Australian Paramedics Association (NSW), Natural Hazards Research Australia, NSW Rural Fire Service Association and the NSW SES Volunteers Association. I am responsible for the content in this post including any errors or omissions. Any opinions expressed are mine, and do not necessarily reflect the opinion or understanding of the donors.